
Clinical Guide for Creating Return-to-Run Programs


The purpose of this guide is to provide pertinent information for both clinicians and running coaches when guiding an injured runner back on the road, track or trail. In the age of offshoring clinical reasoning to artificial intelligence there lies a great impulse for all of us to rely on a generic return-to-run program (R2R). However this use comes at a cost; important information may be missed or misinterpreted leading to worse outcomes. Anecdotally, there is often a disconnect in dialogue between the clinician and coach that may lead to unnecessary prolongation of injury, disruption of training and frustration between all involved. In an effort to bridge this gap, there are several significant concepts one should consider when creating return-to-run programs.
1- Musculoskeletal injuries vary by biological tissue and mechanical stress (based on anatomical location). Thus a R2R program should vary according to frequency, intensity (speed), type and time to reflect these differences. Consider a 5km runner afflicted with an insertional Achilles tendinopathy (iAT) versus an ultratrail runner suffering from distal iliotibial band syndrome (dITBS) versus a runner with bilateral knee osteoarthritis, would one R2R program be sufficient to treat all three runners? What should the runner with iAT avoid? What about the one with dITBS? When you start taking some time to think about the underlying biology and how different tissue types respond differently to mechanical stress you may start to understand why addressing speed, volume, terrain, and frequency is important.
2- There are large temporal differences in the onset of pain for different musculoskeletal injuries. For example fasciopathy has been found to densify in nociceptors, tendinopathies have impaired fluid accumulation and dysfunctional homeostasis and cartilage pain depends whether innervated subchondral bone is involved.
3- What is the runner’s mechanical profile (ground contact time, cadence, vertical oscillation…etc)? What running shoes are they cycling through long distance runs, interval training and race day? Are they supplementing their race-build through cross-training, another sport, or strength training?
Scientific and Clinical Rationale
Below is a brief review supporting my argument for each clinician to consider the three questions above when creating a walk-run program. One of the key ideas of walk-run is the concept of intervals or interval-training. You may be familiar with a type of running known as fartlek. This word is Swedish and translates aptly to speed play implying the runner is granted the freedom of modulating their speed and consequently the magnitude of mechanical stress imparted on tendons, bones, muscles…etc of the lower limb. The question then becomes: Is there scientific evidence supporting the use of intervals?
Two studies between 2014-2015 found that interval training had odds ratios of .61 (CI .43 to .88) and .67 (.33-.81). In English that means that the studies showed that interval training actually acted as a protective measure. Runners who included intervals were roughly one-third less likely to get injured compared to those who didn’t and since our confidence intervals (CI) stayed well below the break-even point of 1, we can be very sure this wasn’t just a fluke finding.
Mechanical Factors
Biomechanical can be found in a meta-analysis by Demangeot et al. in 2022 whereby the load placed on one’s Achilles tendon does not progress linearly implying that small increases in speed can drastically increase the stress imparted on the tendon. Whether this spike in stress leads to more injury remains to be seen in research (2018, 2022 & 2023) , but clinically I would not recommend continuously training at a high pace. This non-linear trajectory of pace versus stress also applies to the patellofemoral joint and the tibia as seen recently in a 2024 study by Bas van Hooren et al. Furthermore, you can see in this study how gradients (uphill and downhill) affected the joints as well. Based on this data you can conclude for a current state of tissue homeostasis there is potentially a red line in which crossing it (via training or race demands) will lead to a running injury. Therefore it is important to employ both fluctuations in training speed to stimulate tissue adaptation (so you can perform better) but to also ensure the tissue is sustainable enough to allow you to continue to run and perform your daily activities. A simplistic model of this can be seen in figure 3.
Now that you understand how the variables of speed and gradients can affect tissue strain and stress it is important you understand how different tissues respond to these mechanical variables. Tendons, muscles, bones, and cartilage are inherently different from one another. I will briefly go over some interesting research for tendinopathies and bone stress injuries to help you understand the differential responses to running.
Biological Factors
Tendinopathies
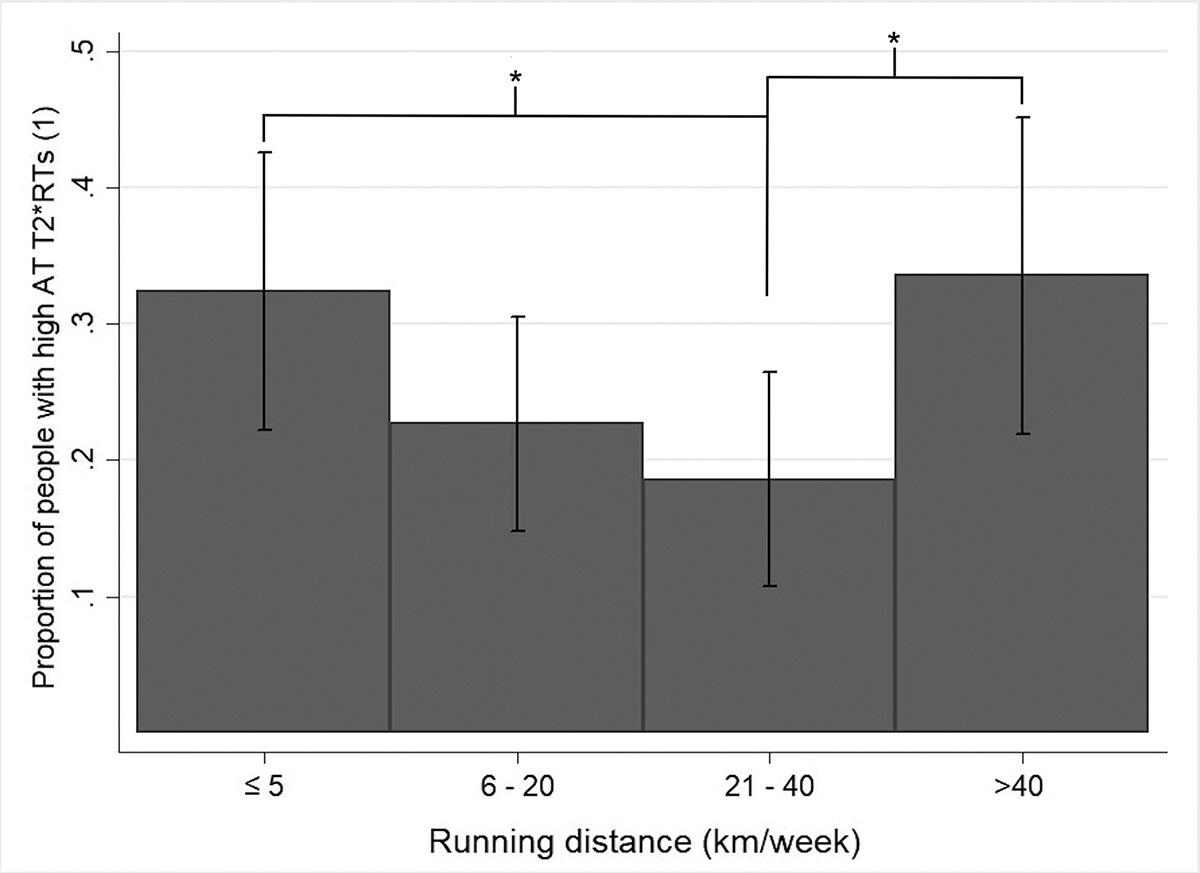
Recent cadaveric 2024 research by Pringels et al. demonstrate that repeated loading the Achilles tendon with tendinopathy leads to significantly higher fluid accumulation compared to a healthy control. For the same amount of strain (2%) the healthy tendon had 25 mmHg of fluid versus the one with tendinopathy had 100 mmHg of fluid. These differences are due to the maladaptive increases in glycosaminoglycan proteins (GAG) and decreasing fluid permeability in the tendon. This may explain an injured runner’s description of how their tendon feels like it is swelling and painful after activity, and particularly speed work. Fluid accumulation takes time and afterwards it compresses against the extra nerve endings within a tendinopathy. A review by Magnusson et al. 2010 highlights how collagen proteins have a net-loss period of 24-36 hours post-exercise suggesting that insufficient rest from tendon loading may increase the risk of damage to higher loads. A recent 2023 MRI study of 350 runners by Jandacka et al. showed that both inactive runners <150 min/week and runners with >40 km/week had the longest T2 relaxation time indicating higher fluid accumulation. All participants in this study were healthy runners and had no tendinopathy, reported no pain but it is interesting to see how the significant differences in fluid accumulation may indicate some maladaptation taking place either in the inactive runners placing an abrupt higher demand on their tendon’s capacity, and with the higher volume runners having potentially insufficient recovery for collagen turn-over to be completed. Based on this evidence you can see the need to modulate frequency/volume and speed to ensure an injured runner with tendinopathy is able to self-monitor and successfully create micro-adaptations to transition from an injured state back to the road.
Bone Stress Injuries
The same logic and reasoning applies to bone remodelling for bone stress injuries (BSIs). The seminal paper by Warden, Edwards and Willy, 2021 declare an uncomfortable truth about running “Distance running does not build good bones” sourcing their reasoning from a 2002 animal study by Burr, Robling and Turner and an epidemiological study by Rizzone et al. 2017. Distance runners have the higher incidence of stress fractures out of any sport but also have some of the lowest bone loading stimuli being lower than soft-ball and tennis. What is the biology behind this? Because the running tends to load the axial bones linearly and uni-directionally the osteocytes actually become deaf and decoherent after a few minutes of running, decreasing adaptations for a stronger skeleton and potentially depleting bone mineralization even in the presence of progressive overload. High volume, high speed running therefore significantly increases the risk of BSIs. The solution? Cross-training with multidirectional sports, plyometrics to avoid bone decoherence and periodize with intervals. Since bone is well vascularized and with lots of nerves, BSIs are very painful and pain occurs immediately. Walk-run intervals are the cornerstone of rehabilitating BSIs and it is important every clinician takes a cautious role involving other physicians and imaging to ensure proper healing is taking place.
Figure 1
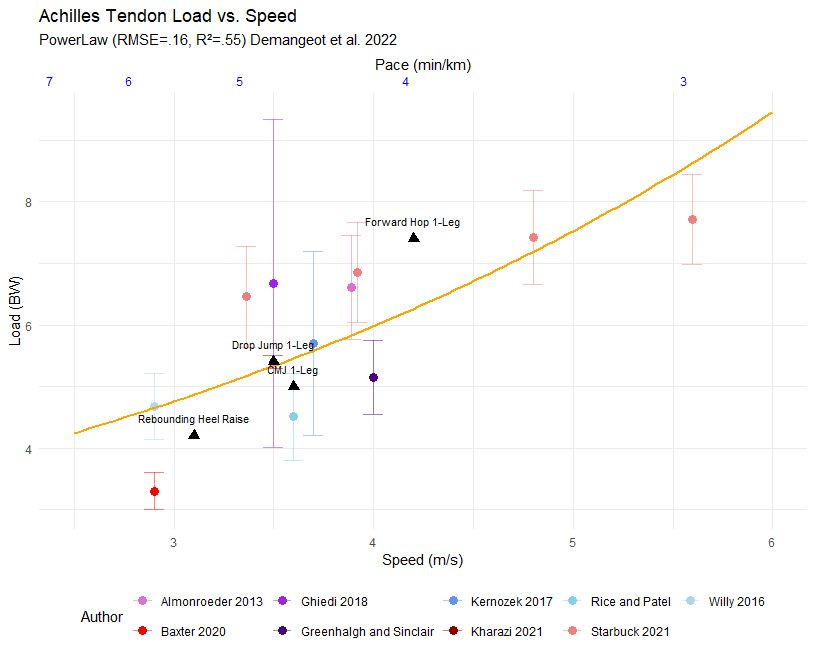
Figure 2
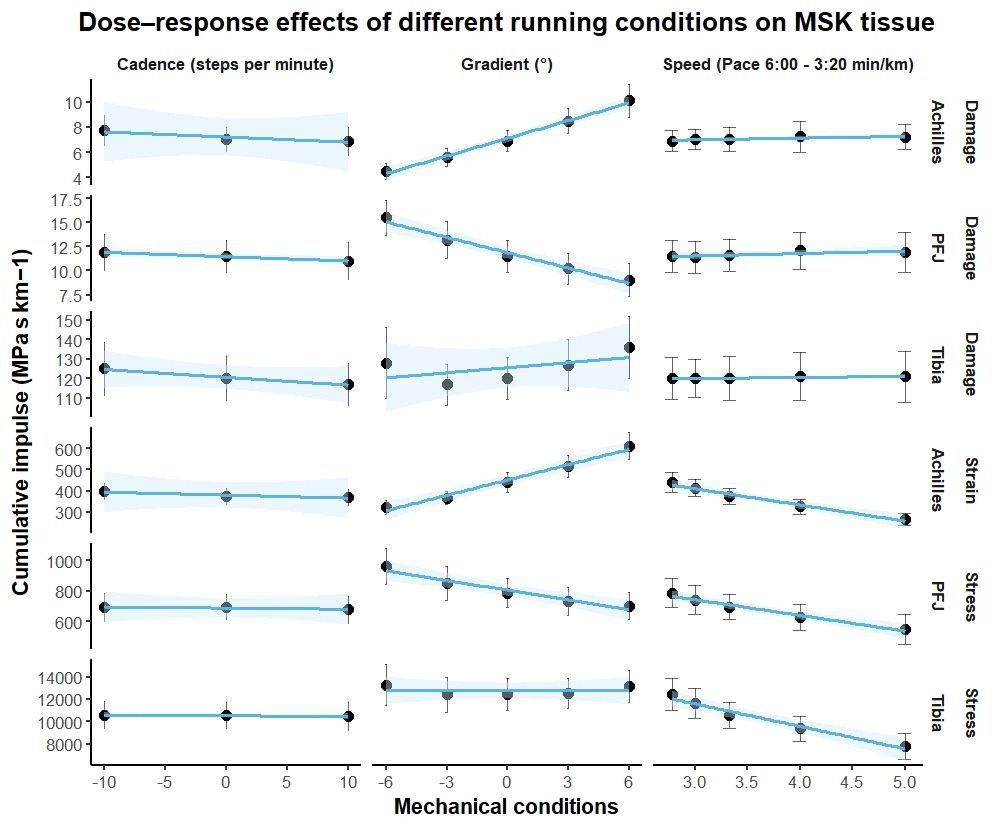
Figure 3
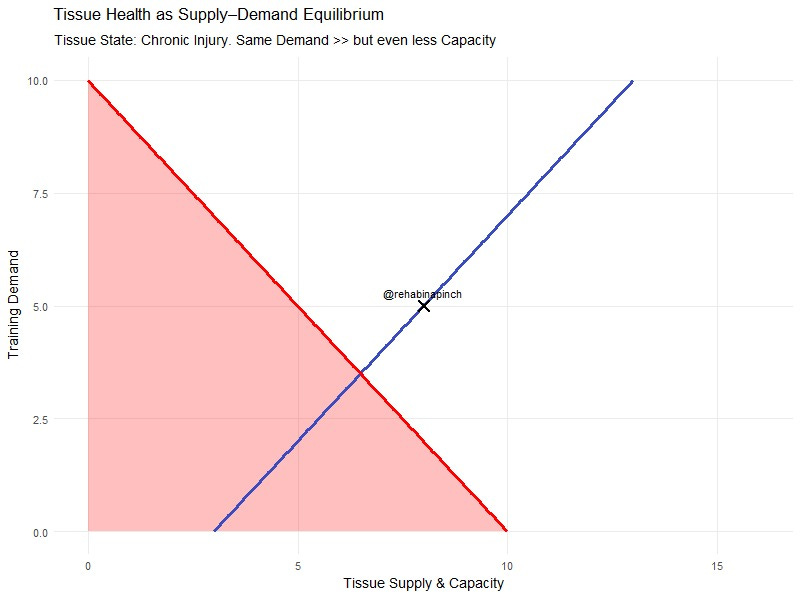
Figure 4
{kind=link}
Click on text for clarity…
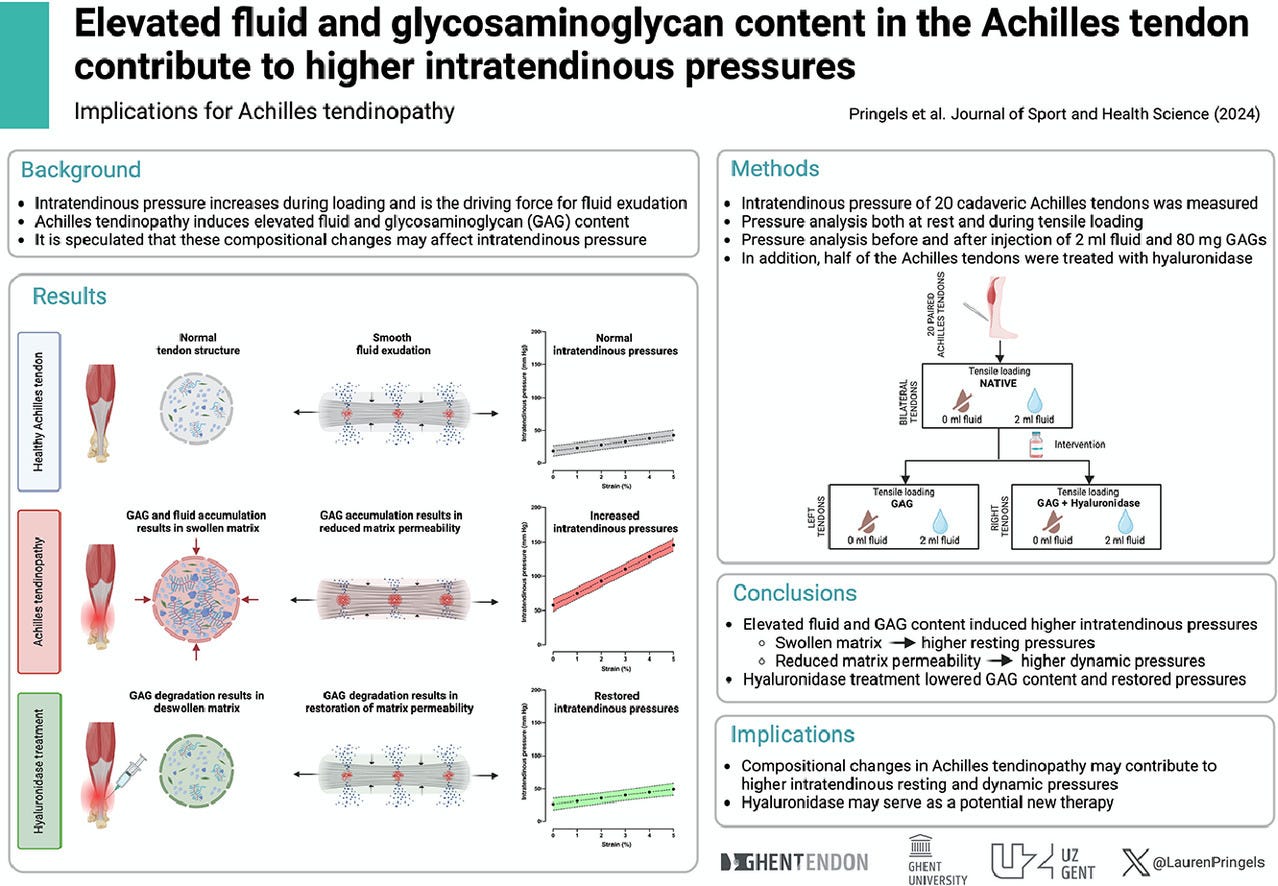
Figure 5
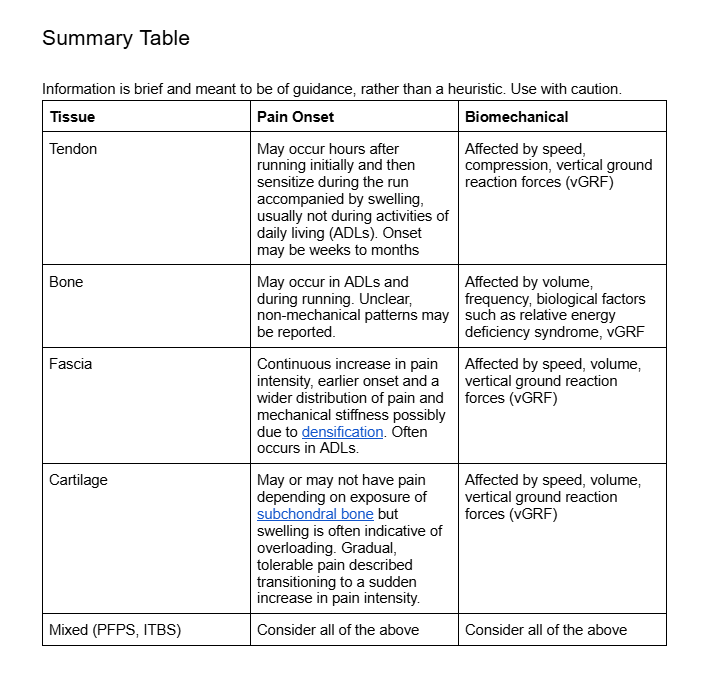
Summary Table
References:
van Poppel, D., De Koning, J., Verhagen, A. P., & Scholten‐Peeters, G. G. M. (2016). Risk factors for lower extremity injuries among half marathon and marathon runners of the L age L anden Marathon Eindhoven 2012: A prospective cohort study in the Netherlands. Scandinavian Journal of medicine & science in sports, 26(2), 226-234.
Junior, L. C. H., Costa, L. O. P., & Lopes, A. D. (2013). Previous injuries and some training characteristics predict running-related injuries in recreational runners: a prospective cohort study. Journal of Physiotherapy, 59(4), 263-269.
Demangeot, Y., Whiteley, R., Gremeaux, V., & Degache, F. (2023). The load borne by the Achilles tendon during exercise: A systematic review of normative values. Scandinavian journal of medicine & science in sports, 33(2), 110-126.
Van Hooren, B., van Rengs, L., & Meijer, K. (2024). Per‐step and cumulative load at three common running injury locations: The effect of speed, surface gradient, and cadence. Scandinavian Journal of Medicine & Science in Sports, 34(2), e14570.
Damsted, C., Glad, S., Nielsen, R. O., Sørensen, H., & Malisoux, L. (2018). Is there evidence for an association between changes in training load and running-related injuries? A systematic review. International journal of sports physical therapy, 13(6), 931.
Dillon, S., Burke, A., Whyte, E. F., O’Connor, S., Gore, S., & Moran, K. A. (2023). Running towards injury? A prospective investigation of factors associated with running injuries. PLoS One, 18(8), e0288814.
Peterson, B., Hawke, F., Spink, M., Sadler, S., Hawes, M., Callister, R., & Chuter, V. (2022). Biomechanical and musculoskeletal measurements as risk factors for running-related injury in non-elite runners: A systematic review and meta-analysis of prospective studies. Sports medicine-open, 8(1), 38.
Pringels, L., Van Valckenborgh, G. J., Segers, P., Chevalier, A., Stepman, H., Wezenbeek, E., ... & Vanden Bossche, L. (2024). Elevated fluid and glycosaminoglycan content in the Achilles tendon contribute to higher intratendinous pressures: Implications for Achilles tendinopathy. Journal of sport and health science, 13(6), 863-871.
Magnusson, S. P., Langberg, H., & Kjaer, M. (2010). The pathogenesis of tendinopathy: balancing the response to loading. Nature Reviews Rheumatology, 6(5), 262-268.
Warden, S. J., Edwards, W. B., & Willy, R. W. (2021). Preventing bone stress injuries in runners with optimal workload. Current osteoporosis reports, 19(3), 298-307.
Burr, D. B., Robling, A. G., & Turner, C. H. (2002). Effects of biomechanical stress on bones in animals. Bone, 30(5), 781-786.
Rizzone, K. H., Ackerman, K. E., Roos, K. G., Dompier, T. P., & Kerr, Z. Y. (2017). The epidemiology of stress fractures in collegiate student-athletes, 2004–2005 through 2013–2014 academic years. Journal of athletic training, 52(10), 966-975.