
Case Study: Runner with Persistent Lateral Hip Pain
Lateral hip pain often entails a complex assessment and treatment plan. Is there a way to simplify the chaos?

Introduction
Lateral hip pain may account for up to 20% of all reported injuries in athletes and characterized by persistent symptoms that last between 6-12 months. The complex anatomy and involvement of multiple tissue structures make the lateral hip a diagnostic and treatment headache for many clinicians as there is a high rate of re-injury post-treatment. In this two part series, we will explore the current literature for an evidence-informed approach of assessing and treating lateral hip pain in a runner from a 2013 case study.

Case Presentation:
A 30 year old female distance runner presents complaining of persistent left posterior hip pain extending to the outer hip regions. The initial injury occurred four months prior during a trail run when she tried to avoid falling. Despite immediate proximal hamstring pain, she completed the run but couldn't tolerate speed work afterward. Self-treatment with NSAIDs, ice, and gentle hamstring stretches which provided temporary relief. Then significant exacerbation of pain occurred six weeks later after prolonged sitting, leading to localized pain and tingling along the hamstring. The patient then reduced running, switched to pool training, and completed a marathon but required multiple bouts of walking throughout.
”The patient completed a numeric pain rating scale for pain and rated her worst pain as 7/10 when sitting more than one hour or attempting to run hills or run at a faster speed. Pain was noted in the left gluteal region, ischial tuberosity and pubic ramus with speed walking or running, particularly at the point of initial contact of the left lower extremity. The pain reported with running was not consistently reproducible and was most intense during the first several miles of a run which reduced if attempts were made to shorten her stride length. She experienced periods of no pain (0/10) with rest and casual walking but began to notice some pain while sitting (2/10) that would improve with slight movements or changes in position. The patient's goals were to resume running and tolerate sitting without pain.” -Podschun et al. 2013
In the last week prior to seeing you, she had completely stopped running, experienced pain with sitting, and reported aching and burning at the left sit bone with diffuse discomfort in the hip region. Past medical history is not significant for any medications or injuries. What is your problem list? And what would you do for your assessment of this runner?
Problem List:
a. Persistent and increasing load intolerance/pain
b. Diagnostic challenge due to regional interdependence
c. Ongoing deconditioning due to pain at rest and minimal activity

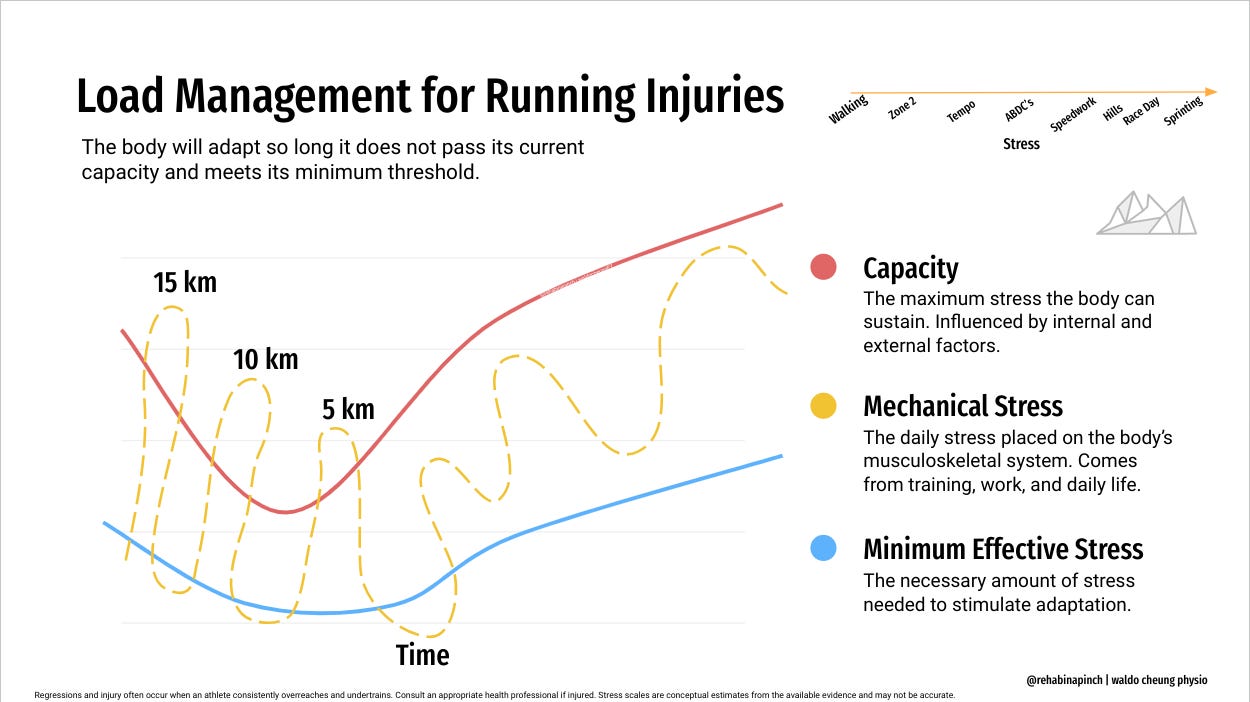
Running History
Within the runner’s subjective history, she already describes a diminishing capacity over the last several months prior to her initial visit. She also included which running workouts generated pain (hills, and speedwork). This should clue the clinician to figuring out what sort of maladaptive (overloading and underloading) stress she has been applying to her body. It should also help with the correct prescription of run/walk programs and exercise programs to improve the runner’s stress capacity and resilience. Now there may be many reasons for a decreasing capacity including some red flags and concerning pathologies we need to rule out. But make note of this first before your physical assessment and you can circle back to it for education and treatment.
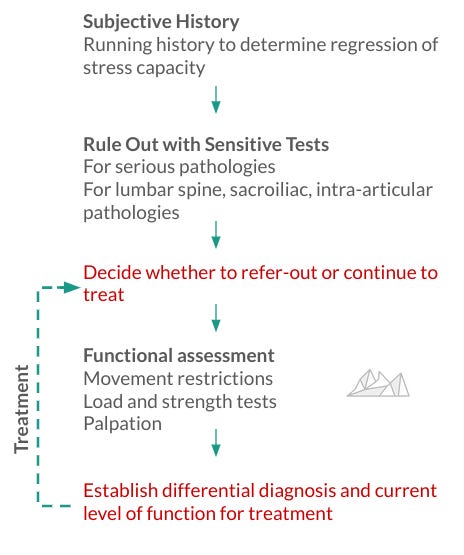
Rule-Out Algorithm
A systematic way of ruling out serious pathology affecting the hip can be done via assessing for the following: red-flags, stress fractures, lumbar pathology and pelvic-girdle pathology. The results here should indicate whether the clinician should refer for medical consultation or begin treatment. We will be using probability and likelihood ratios as it is especially vital in medicine and physiotherapy. Remember test sensitivity is for ruling out a condition, and specificity is for ruling in. Likelihood ratios (LR) are a way of determining the impact of a test based on its sensitivity or specificity. You may have a high sensitivity or specificity, but if its LR is small it may not change the probability of that condition existing or not.
Red Flag Screening
Screening questions: Is there unexplained and significant weight loss over the last 6 months (i.e >10 lbs)? Was there trauma to the area, prolonged NSAID use or fever? Are there issues with incontinence or pain with continence?
Rationale: The hip and pelvic girdle are common areas where primary cancers may metastasize. Inguinal hernias and chronic pelvic pain may also mimic musculoskeletal pain.
Case Report Findings: The runner’s past medical history with her physician and specialists suggest no concern for non-musculoskeletal causes of pain.
These vital questions are easy to ask but often missed as the therapist can be biased towards a musculoskeletal source of pain based on the runner’s story. If the overall functional assessment is confusing and inconclusive, it may be helpful to the therapist to ask these questions again as these medical questions may be sensitive for the client.
Rule Out Stress Fracture of the Hip
As our runner is of female sex and runs marathons this increases her risk of a stress fracture. Remember a history of the runner’s weekly mileage and intensity should also help with screening for hip fractures. Be sure to identify high risk stress fractures on the femoral neck (supero-lateral) and diaphysis, low risk stress fractures in this area are the sacrum, infero-medial side of the femoral neck and pubic rami (May and Marappa-Ganeshan 2023).
Fulcrum Test: Carries a sensitivity of 88-93% with a -LR of .09 indicating a decrease of ~45% chance of a stress fracture if negative.
Description: Runner is seated on a table and the clinician places their forearm under the affected thigh. The free hand is then placed on top of the quad and pressure is applied downward to mimic a bending motion on the femur.
Case Report Findings: The runner tested negative for the Fulcrum test and did not reproduce any painful symptoms indicating a low probability of a stress fracture.
Note: A positive finding does not mean you need to stop treating the patient, but referral to a sports physician for clarification and support may be helpful. A trained therapist can treat a low risk stress fracture with a run/walk program with gentle loading that is pain-free. Based on the negative Fulcrum test, the runner likely does not have a stress fracture.

Rule Out Lumbar Pathology
What about the lumbar spine and facet joints? How do we rule out their involvement? A standard neural screen using myotomes/dermatomes (L2-S2), deep tendon reflexes and clonus and Babinski may help rule out central pathologies versus peripheral nerve lesions. This may be indicated due to our runner’s subjective history but the lack of pain when walking and pain when resting does not fit with the neural picture. The runner passed the neural screen but it does not rule out lumbar pathology. Below are some sensitive tests to use.
ROM with Repeated Motions: Carries a Sensitivity 92%, -LR .12
Description: The runner is standing and repeating forward bending and extending of the spine to reproduce pain. This can also be done with bending side to side.Case Report Findings: Restricted in flexion due to tension in the hamstring. All other movements were pain-free and within functional limits. A high sensitivity coupled with an impactful -LR suggests that the lumbar spine may not be involved with the lateral glute pain.
Seated Extension + Rotation: Carries as 100% sensitivity, and -LR of .0 (near)
Description: The runner is seated while the clinician stabilizes the sacrum and passively moves the spine extension and rotation. Over-pressure may be applied if there is no pain.
Case Report Findings: A negative test for the runner. This test is highly sensitive and making a negative finding is near conclusive of ruling out lumbar pathology.Straight Leg Raise (SLR): Carries a sensitivity of 97% and a -LR of 0.05 . A specificity of 57% and a +LR of 2.56
Slump Sit Test (Slump): Carries a sensitivity of 83% and specificity of 53% and a -LR of .3 and a +LR of 1.76
Description of the SLR and Slump: The runner lies supine and the clinician passive lifts, adducts and medially rotates the leg while the knee is straight. Looking for reproduction of the symptoms that are relieved with decreased hip flexion but increased with neck flexion. This can also be done seated.
Case Report Findings: Both reproduced pain on the hamstring and back. High sensitivity and moderate -LR. This is a positive finding so it may indicate lumbar involvement. Read more below.
The pain with the positive SLR and Slump does not mean that the runner has referred pain. The pain could also be from the increased hamstring tension leading to sciatic nerve irritation near the piriformis or the adductor magnus near the ischial tuberosity. Remember these tests are for RULING OUT lumbar pathology not ruling in. Based on the negative findings from ⅔ tests, the probability of lumbar involvement for the patient’s symptoms and signs is low.

Rule Out Pelvic Girdle Pathology
After 2005, the literature appears to have moved on from Laslett’s Cluster due to its operator dependence and decreased sensitivity/specificity compared to other tests. So how do we determine the influence of the sacroiliac joint or pelvic girdle? Also remember that piriformis is a key muscle in the pelvic girdle! We may often forget it as it originates from the anterior sacrum, but its involvement with the sciatic nerve and runner’s history does require it to be ruled out.
Thigh Thrust: Carries a sensitivity of 74-88% and -LR .18 and a specificity of 44% and +LR of 3.6 (a moderate impact test).
Description: The runner is lying supine and the clinician places their hand towards the tail of the sacrum and flexes the hip to be at 90 degrees, then force is applied onto the femur and towards the hip for 3-5 thrusts or 30 seconds to see if pain is reproduced. This test is very delicate so please caution and explain to your runner what you are doing!
Case Report Findings: Runner tested positive on the thigh thrust test but only has a low specificity and a moderate +LR.FABER: Carries a sensitivity of 71.8% and -LR .33
Description: The runner is lying supine and the affected leg is moved passively into flexion, abduction, and external rotation onto the other knee. The therapist then pushes down to see if pain is reproduced.
Case Report Findings: Runner tested negative on this which has a moderate -LR.
Note: Nejati et al. 2020 reported that a combination of the Thigh Thrust and FABER has a sensitivity of 72% and a specificity of 66%, a +LR of 2.1 and -LR .42 (these are small impact tests).FAIR: Carries a sensitivity of 88% and -LR .14 and a specificity of 83% and +LR of 5.2
Description: The runner is lying supine and the affected leg is moved passive into flexion, adduction, and internal rotation onto the other side of the hip. The patient is resisting the internal rotation and adduction by pushing out via contracting the piriformis. A positive test reproduces pain that may radiate.Case Report Findings: Runner tested negative on this
Based on these results, it is inconclusive to rule out pelvic girdle pathology as a possible contributor to her symptoms. In this case we can make a note of this and include the SI joint as part of our treatment plan.
Ruling Out Intra-Articular Pathology
How do we know if the labrum is torn, or if there is a cam or pincer impingement of the femoral head and acetabulum? This area and tissue type is articular as it describes the joint and cartilage. To rule this out we use the FADIR test
FADIR: Sensitivity 99%, -LR .15
Description: Runner is lying supine and the affected leg is moved passively into flexion, adduction and internal rotation. Therapist is looking for reproduction of pain.
Case Report Findings: Runner tested negative on this. Due to the high sensitivity and moderate to high impact (~30-45% decrease). It is unlikely that the runner’s symptoms are coming from the hip joint.
Now that we have ruled out the lumbar and hip joints, and noted the pelvic girdle. We can move into a functional assessment of the hip. While there are tests for ruling in articular hip pain (the Ligamentum Teres and Modified Thomas Test), it does not exclude the involvement of the muscles, tendons and irritated nerves around the lateral hip. My question to you is this, “does ruling in different structures of the lateral hip change your management?”
As discussed in previous posts, the objective examination by the clinician may have little diagnostic value but yield highly valuable information for establishing a baseline for physiotherapy. Understanding the painful limitations of range of motion, and loaded movements will optimize healing and return-to-running for the patient.
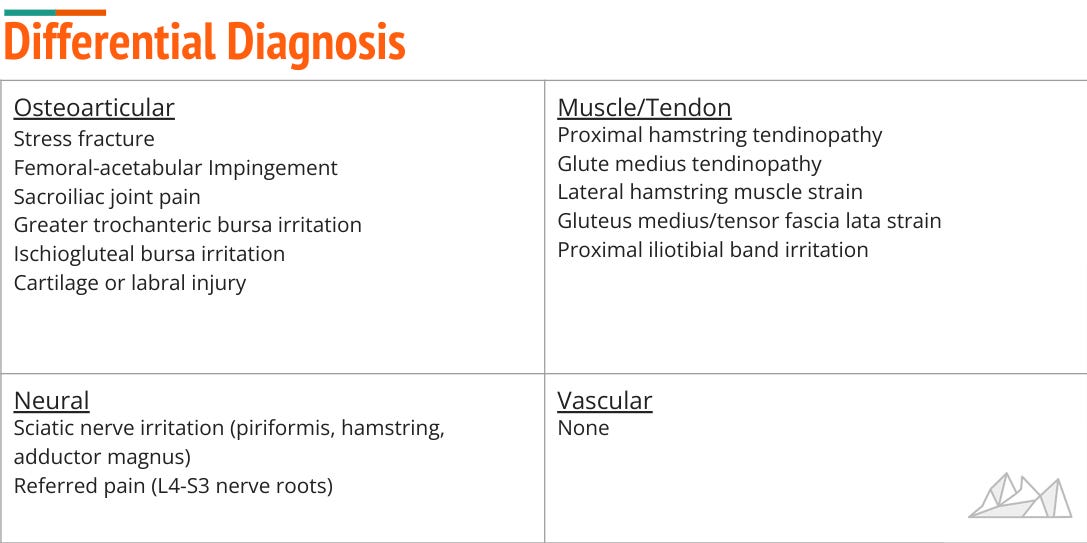
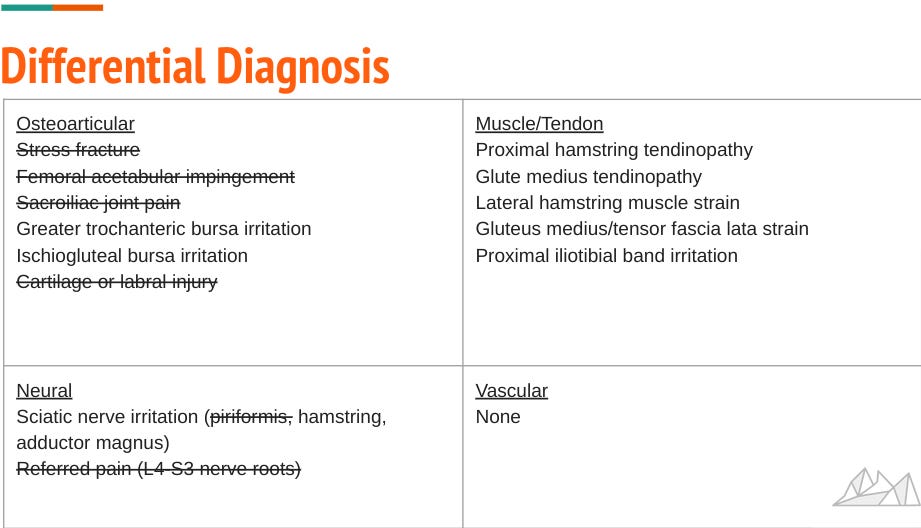
Differential Diagnosis
You can see how our runner initially had a myriad of possible diagnoses (13, if not more). With our algorithm we have eliminated close to 50%. The bursa, muscle and tendon diagnoses should not be too difficult for an experienced physiotherapist to identify using a combination of load/strength testing and palpation. If there is concern of misdiagnosis within these 7 structures, ask yourself this question “Does my management significantly change if it is a glute medius tendinopathy versus hamstring tendinopathy?” Given that there should be reassessment and follow-up treatment sessions there is always time to fine-tune which exercises and treatment techniques to use but more serious pathologies that require referral should always be ruled out first.
Movement Deficits
A 2018 consensus statement in Zurich by Mosler et al. recommended that hip range of motion be tailored to the goals and needs of the individual. There is evidence by Dobson et al. 2012 and by experts on the consensus statement arguing whether range of motion, posture and leg length is relevant to managing a patient with hip pain. This is because ROM measures can be highly unreliable and variable depending on the inherent anatomy of the patient.
Case Report Findings: Some mild tightness was noted on both hips and quadriceps, especially during a Modified Thomas Test. But there was no clicking, popping or significant painful restrictions of the left hip in active or passive movement.
In general, any restrictions should be noted if there is pain and this can be used as a comparative measure in the future.

Load versus Strength Testing
While decreased muscle strength has been identified in several studies in athletes with hip pain and correlated with different pathologies such as arthritis, the methods used via resisted isometrics and manual muscle testing (MMT) is limited. The literature concludes that quantifying strength past 3/5 (which is moving against gravity) yields little information. So the overall utility of a 4+/5 vs 4/5 vs 5/5 may not be useful as most outpatients and runners have greater than 3/5 strength. What is useful is the varying amounts of pain reported from the runner as each muscle test biases activation levels of muscles. More pain could indicate a lesion in the muscle or tendon.
Case Report Findings:
Strength testing yielded the following
Gluteus maximus: (tested prone with knee bent): 4/5 bilaterally with pain on left (2/10)
Hamstring: (tested prone with resisted knee flexion): 4+/5 painful on left (2/10)
Hamstring: (tested supine with left hip flexed to 90 degrees and terminal knee extension): 4/5 on left with significant increase in reported pain (6/10)
Important Note: The case report authors did not employ any load testing such as moving from single leg stand, single leg squat, single leg hop. I would highly suggest using these tests as they are functional and relevant to running. As running a series of propulsive hops, these tests should be used as outcome measures and indications for a return-to-run regimen.
Loading Tests:
1. Single Leg Stand for 30 seconds- 100% sensitivity and .0 -LR , 97.3% specificity & +LR 33.3
2. Bilateral supine bridge —> Side Lunge —> Single Leg Bridge —> Hopping or Jumping. Evidence is not diagnostic but can help quantify the amount of load capacity the muscles and tendons can take for treatment as per Mellor et al. 2018.
What about Palpation?
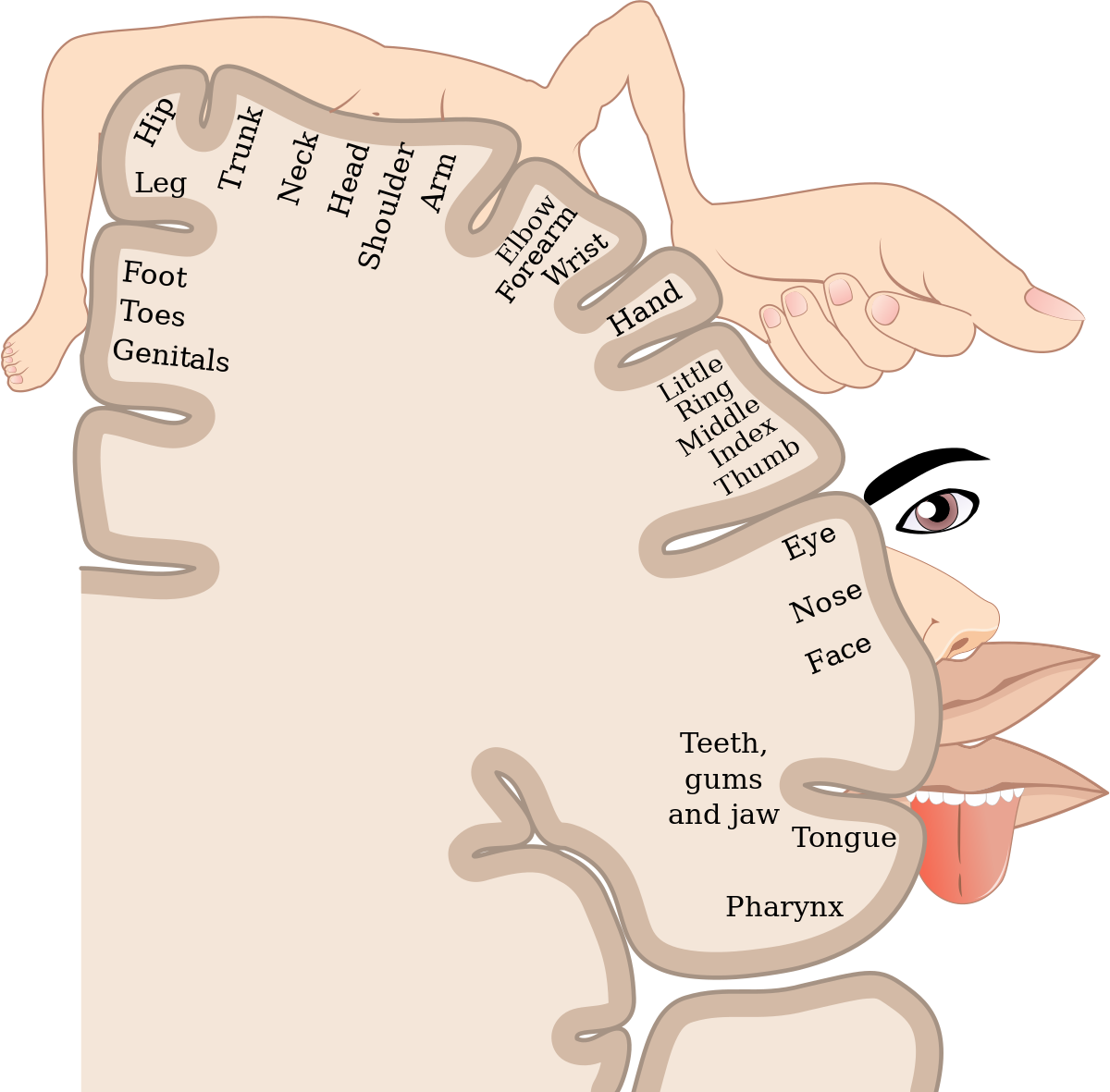
The freakish picture below is the homunculus which is a visual representation of the somatosensory cortex. A larger body part is proportional to the amount of sensory feedback inputted to the brain meaning that point palpation towards the hand and its individual fingers are highly specific and accurate. What about the hip? You can see that it owns a very small portion of its cortical real estate making it difficult for the mind to parse between the gluteal tendon, bursa, or iliotibial band. There is evidence from Kinsella et al. 2023 that painful palpation of the greater trochanter and painful resisted abduction increased the probability of greater trochanteric pain syndrome from (59% to 96%). But the greater trochanter is still very vague regarding the different structures inheriting that area, as mentioned above. As palpation is operator dependent and has a low reliability (kappa < .4 meaning 4-15% of the data is reliable), one should be cautious when making a sole diagnosis from palpation. You can narrow down the affected area with palpation but be transparent to all the different structures that could generate pain.
Case Report Findings: Tenderness on palpation included the left pubic ramus, the left ischial tuberosity and proximal bicep femoris tendon. Note that the authors include several areas that are tender not just one.
Comparison of Assessments
Podschun et al. 2013 report the following diagnosis, “the primary working diagnosis was hamstring syndrome. Hamstring syndrome has been described as a gluteal sciatic pain in which there is irritation of the sciatic nerve due to scarring or fibrosis of the tendinous origins of the proximal hamstring muscles at the ischial tuberosity, often due to recurrent strains or partial tears of the proximal tissues.”
My diagnosis: “30 year old female presents with persistent left hip pain with regressing capacity to run over an hour, run hills or perform speed work without pain. Pain is present when sitting, and running but not walking and radiates from glutes to the outer hip. Based on the patient’s history, the ruling out of other pathologies and focal reproduction of pain from contracting the proximal hamstring and palpation along the ischial tuberosity, the working diagnosis could be irritation of proximal hamstring and adductor muscles (biceps femoris and adductor magnus), tendon and sciatic nerve.”
Critique: While the Podschun et al. did a good job with their tests and subjective, they could have utilized some load tests and included a few outcome measures such as Copenhagen Hip and Groin Outcome Score (HAGOS) and the International Hip Outcome Tool (iHOT-12). The measures are valid, reliable and have normative data relevant to athletes returning to sport.
Summary
The case emphasizes the importance of identifying the interdependent pain generators causing proximal posterior thigh and gluteal symptoms. Anatomical models that separate the lumbar spine, pelvis, and legs may not account for the complex coupling of these structures from a neurophysiological, biomechanical, and functional view. While imaging is often concurrent with assessment, it does not change management (unless a serious pathology is detected).
Lateral hip pain in runners is challenging to assess so rule out serious pathologies, refer out if needed and take a history of the runner’s load capacity. In part II we will delve into the details of optimizing this patient’s rehabilitation and how the patient successfully returned to running a weekly distance of 22 miles and racing marathons again.
References:
May, T., & Marappa-Ganeshan, R. (2022). Stress fractures. In StatPearls [Internet]. StatPearls Publishing.
Podschun, L., Hanney, W. J., Kolber, M. J., Garcia, A., & Rothschild, C. E. (2013). Differential diagnosis of deep gluteal pain in a female runner with pelvic involvement: a case report. International journal of sports physical therapy, 8(4), 462.
Reiman, M. P., & Thorborg, K. (2014). Clinical examination and physical assessment of hip joint‐related pain in athletes. International journal of sports physical therapy, 9(6), 737.
Kinsella, R., Semciw, A. I., Hawke, L. J., Stoney, J., Choong, P. F., & Dowsey, M. M. (2024). Diagnostic accuracy of clinical tests for assessing greater trochanteric pain syndrome: a systematic review with meta-analysis. Journal of Orthopaedic & Sports Physical Therapy, 54(1), 1-24.
Mosler, A. B., Kemp, J., King, M., Lawrenson, P. R., Semciw, A., Freke, M., ... & Lewis, C. L. (2019). Standardised measurement of physical capacity in young and middle-aged active adults with hip-related pain: recommendations from the first international Hip-related pain research network (IHiPRN) meeting, Zurich, 2018. British journal of sports medicine.
Nejati, P., Sartaj, E., Imani, F., Moeineddin, R., Nejati, L., & Safavi, M. (2020). Accuracy of the diagnostic tests of sacroiliac joint dysfunction. Journal of Chiropractic Medicine, 19(1), 28-37.
Nolet, P. S., Yu, H., Côté, P., Meyer, A. L., Kristman, V. L., Sutton, D., ... & Lemeunier, N. (2021). Reliability and validity of manual palpation for the assessment of patients with low back pain: a systematic and critical review. Chiropractic & manual therapies, 29(1), 33.
McHugh, M. L. (2012). Interrater reliability: the kappa statistic. Biochemia medica, 22(3), 276-282.